
Alright – so today we’ve got the honor of introducing you to Phoenix Aka “mohawk” Kellye. We think you’ll enjoy our conversation, we’ve shared it below.
Phoenix AKA “Mohawk”, thanks for taking the time to share your stories with us today Can you open up about a risk you’ve taken – what it was like taking that risk, why you took the risk and how it turned out?
Harm reduction is a controversial and commonly misunderstood movement fraught with challenges. While the movement has garnered a lot more support over the last seven or eight years (due to fentanyl, xylazine, and other toxic and deadly adulterants running rampant through some of the drug supply), services as basic as syringe exchanges are considered illegal in many places, and mainstream stigma and carceral or other punitive laws around drug use and distribution creates barriers to enacting positive change. This was especially the case when I started this work in 2012 as a person engaging in drug use seeing both the negative and positive impacts drug use has on people in my community and wanted to find ways to enact positive change without creating more stigma or judgement.
Achieving any success and forward progress in this work has meant tackling more-resourced and influential opposition, even at the expense of my safety and security. There’s nothing glamorous about this work, and even for sanctioned facilities and organizations, the legal protections and protocols for safety are minimal and challenging to enforce. There are people in this work that now carry a permanent felony record for simply engaging in activities that would keep people alive and well. Imagine if all of our research and development of prescribed medications to prevent spread of illness and infectious disease were not regulated and quality controlled, and interventions like STI testing were illegal–this is virtually the level of risk harm reduction workers like myself are up against.
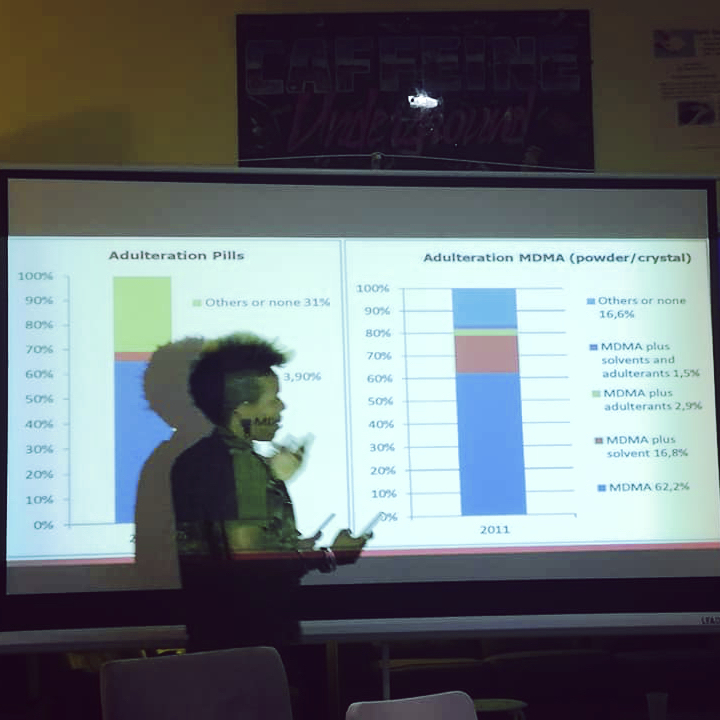
Drug checking services provide data, analysis, and insights on the drug market and the drugs’ contents themselves. This work, which has wide-reaching implications for people who use drugs (PWUD), influences policies, regulations, protocols, service delivery, and PWUD advocacy. Government officials, local agencies, and organizations need data on emerging drug supply trends to initiate appropriate prevention services. However, harm reduction is a movement that was pioneered during the AIDS epidemic in the mid to late 1980s and 90s, when tens of thousands of mostly gay men were dying every day, as the government remained largely indifferent to this public health crisis. The CDC stigmatized the gay community by initially labeling the disease Gay-Related Immune Deficiency (GRID)/”Gay Plague”/”Gay Syndrome” and targeting spaces with “high risk” sexually activity, where gay men primarily congregate until it was discovered that people who inject drugs, Haitians, and people with hemophilia were also contracting the disease.
These activists sought out to help their own community by founding a philanthropy that evolved into Housing Works, which directed resources (including money raised by a chain of thrift shops) toward AIDS services and homelessness, helping establish the first successful needle-exchange programs in New York City, and influenced a fundamental change in the way clinical trials are conducted in the United States. Today, drug candidates for life-threatening conditions are frequently put on a parallel track for “expanded access.” Without the radical work of these activists over the last 40+ years we would not have the framework for the interventions that are used and are still effective today.
Inspired by the the harm reductionists that came the generation before, I felt I was uniquely positioned to expand outreach, having done an incredible amount of networking and capacity building using my background in web engineering, communications, and online media. in October 2019, for my boldest stunt up until that point, I borrowed an FTIR spectrometer from an organization in Chicago and operated a drug checking drop-in out of my apartment for the week and weekend of Halloween. A curious neighbor wanted to see it in action. She is now the Drug Checking Manager at the NYC Department of Health and Mental Hygiene and since 2023, there are five syringe service programs in NYC that have drug checking onsite. I can not be solely credited for initiating drug checking efforts using a spectrometer in NYC–however I was certainly the first here. I took on most of the risk, acquiring illicit substances from all over the city with the help of some comrades, just to prove that this work could be done without issue or interference, with positive outcomes for the community. I also only had only operated a spectrometer supervised on two or three occasions prior to being entrusted with $50,000 worth of equipment that was loaned to me for free, and leaned on the guidance of scientists based in Canada and England to help complex levels of chemical analysis.
In 2022, I was one of the dozen finalists for the David Prize, and I was gifted an FTIR spectrometer of my own by one of the judging participants to advance my work with drug checking. Since receiving this tool in 2023, I have independently been able to reduce some of the barriers to meeting community needs, as spectrometers are typically only available for drug checking through expensive laboratories or at drop-ins in a small number of cities. To date, I have performed drug checking on street drugs in 3 countries in Africa where drug checking does not exist and drug use casualties have, in some cases, reached a state of emergency requiring global humanitarian intervention. I am continuing to research and build capacity to expand access to these services and prevention education beyond what I can provide individually.


Phoenix AKA “Mohawk”, before we move on to more of these sorts of questions, can you take some time to bring our readers up to speed on you and what you do?
I’m Phoenix or Mohawk (they/them), and I’m a tenacious, globe-trotting harm reduction advocate known as the Rebel Educationist.
I learned about harm reduction as a concept fairly early on through organizations like ACT UP NY and DrugsData.org (formerly EcstasyData.org). After a number of traumatic drug-related experiences, I began asking, “When is someone going to do something about all of these overdoses in my community?” In 2012, I realized it was time to become that person myself.
Now, over twelve years later, I am a harm reduction educator and advocate for People Who Use Drugs (PWUD). I provide online educational resources as well as in-person services tailored to each situation, individual, and community I work with. I also analyze emerging drug trends and tracking that may be harmful or lethal so that I can offer preventative health interventions and education.
My work transcends physical borders. I have traveled to many regions of the globe such as Canada, Mexico, England, Sierra Leone, and South Africa, but I maintain a solid foundation for organizing and capacity building in my cherished local community of Brooklyn, NY. I experienced one of the many waves of the opioid and substance use disorder epidemics firsthand in Ohio when I lived there for four years as a young adult, and now, I attend events there such as the Gathering of the Juggalos to both build authentic relationships and provide harm reduction services.
My advocacy work impacts the intersectional communities I belong to, like People Who Use Drugs (PWUD); Black, Indigenous, and People of Color (BIPoC); and LGBTQIA+. The work I do falls within the Participatory Action Research (PAR) framework, which states that research should be done by the most impacted community. PAR is defined as a set of principles and methodologies that centers the people closest to the experience as leaders in research. The framework provides a construct for marginalized communities to envision and enact solutions that will impact their everyday lives. As a Black trans person who both uses and researches drugs, I have an important perspective that helps me identify patterns and issues that many public health researchers in the field lack the personal experience to find.

What do you think helped you build your reputation within your market?
I’m in the “business” of caring for my community. It feels easy because my motivation is just that–not clout, money (if you get into any public health, social work, or activism for the money, you’ll be sorely disappointed), or access to resources. Much of building trust and a reputation is being involved and hands on, authentically interacting with people, and most importantly (in my opinion), delivering on promises. There are parallels to being a politician. If your values and initiatives are not in alignment with the people or community you’re expected to represent and advocate for, you will lose their support. It’s as simple as that, but it didn’t come easy. I still had to convince people to believe in and support harm reduction, which includes not condemning people for their drug use, and supporting their safety and well-being even if they are not on a path to abstinence.
Any advice for managing a team?
I mostly work independently these days, but for the first eight years of this work I managed large teams of dedicated and talented volunteers. I avoided overwhelming them. I made sure they could always opt in/out of the work and gave them ample opportunity to contribute their unique ideas and skills to the work. I also identified any strengths they had, and assigned tasks and responsibilities that would be appropriately challenging and rewarding for them.
I arranged contracts with stakeholders (to the best of my ability) that stayed within the parameters of what these volunteers could realistically do, without putting them in harm’s way, at legal risk, or having their labor exploited when stakeholders would attempt to give too much responsibility to an individual who, by law (at least in New York), should not be doing work that would typically done by a paid employee. Since we are considered peer workers/educators that often had to work with intoxicated individuals, some stakeholders took this to mean that volunteers could stand in as medics, security, or “trip sitters”, who are traditionally volunteers that are also trained and/or licensed specifically to perform those duties.
Many of my volunteers and collaborators were also members of the communities we served, so it was especially important to provide meaningful involvement and growth opportunities. I didn’t feel the need to micromanage anyone or put unnecessary pressure on my volunteers, as the work is already physically and emotionally taxing. We worked onsite, sometimes in extreme hot or cold conditions outdoors or in industrial spaces for days on end, exposing volunteers to injury and illness. Some events required travel, and a number of volunteers may have been in traffic accidents. I always advocated for my volunteers’ safety and security, and if a job proved itself too intense to work again, I would decline out of the best interest for my volunteers.
Many people that do activism and advocacy work struggle to maintain healthy boundaries to not push themselves to the point of burnout. There may have been times when volunteers would be disappointed, but there were many others doing the same type of work around the country and I often heard complaints from those volunteers that they were expected to work an unsustainable amount, or that they felt they had to continue the work even if they were facing instability such as unemployment and/or homelessness. Many of these volunteers that felt overwhelmed volunteering under other harm reduction service providers would enjoy traveling to New York to work events with our team when given the opportunity and I always supported mediation during conflict. In one scenario, volunteers in Philadelphia were struggling to continue their work due to the former volunteer director sabotaging opportunities when they were no longer permitted to be involved. I used my negotiating skills, connections, and my reputation to restore relations between these parties. They continue to operate to this day, and still leverage many of the educational resources I had created during my tenure.
Some of these volunteers continued volunteering or went on to formally work in harm reduction, even if they moved out of New York City or after I retired from volunteering site and volunteer management and event coordination in 2021. Some were inspired to go back to school and change their career, and because the volunteers and any paid staff are community members, it in turned inspired many that they served to get involved in harm reduction as well. If that isn’t cosidered maintaining high morale in a high stress environment–then I don’t know what is!
Contact Info:
- Website: https://therebeleducationist.com/ +++++ and also +++++ https://rebelharmreduction.org/
- Instagram: https://www.instagram.com/therebeleducationist/
- Linkedin: https://linkedin.com/in/mohawkkellye/
- Youtube: https://www.youtube.com/@therebeleducationist
- Other: Open Collective so that people can help fund the work I do: https://opencollective.com/rebel-harm-reduction


Image Credits
The middle photo of me with the microphone at the black table with 2 other folks was shot by Nigel Brunsdon.
https://nigelbrunsdon.com/
The photo of me at the table with the yellow tablecloth speaking to someone in a denim vest was shot by Kate Hoos
https://www.instagram.com/hoosatron/